Why Doesn't Group Health Insurance Cover Dental in India?
Why group health insurance excludes dental in India and what HR teams and brokers should know about structuring real dental coverage for employees.

.svg)



For HR leaders evaluating dental coverage for their workforce, the most useful question isn't "do we have dental in our policy" - it's "which procedures will our employees actually be able to claim, and which will they be told are excluded after the fact." This article walks through the procedure-by-procedure coverage structure that defines well-designed Indian group OPD dental plans in 2026.

*The coverage logic in this article reflects how ToothLens Dental Plans are structured, drawn from operating a network of 1,500+ dental clinics across India. Specific tier coverage, sub-limits and rider availability vary by plan; the underlying clinical and actuarial reasoning is consistent.
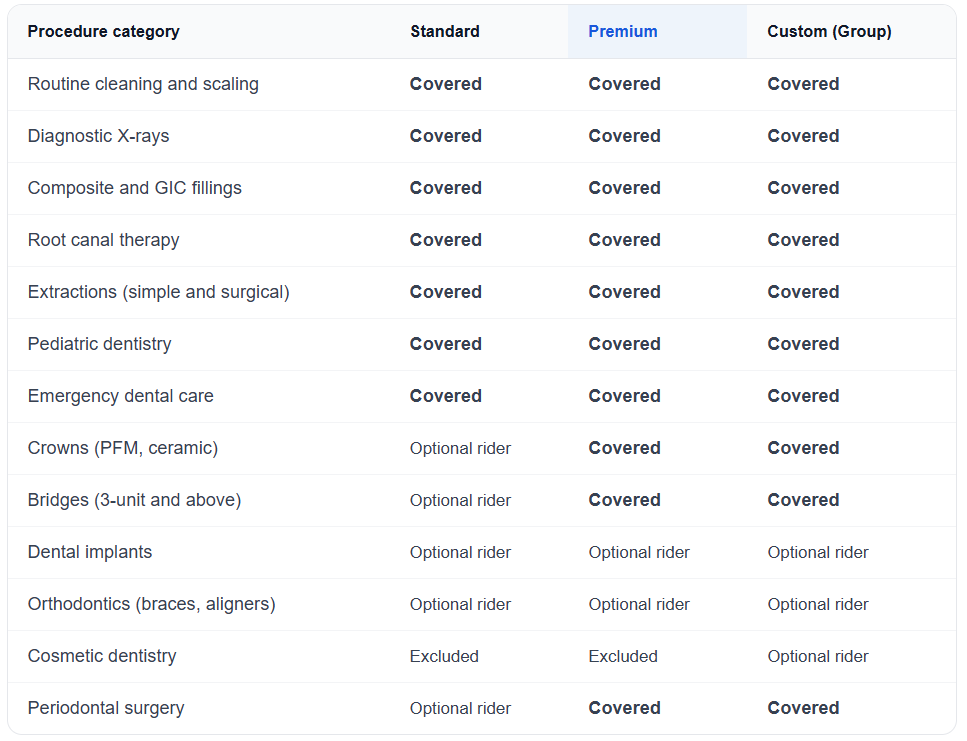
The structure across tiers reflects three principles: preventive care is always covered (employers benefit financially from preventive utilisation), high-frequency restorative care is always covered (this is what employees actually use), and high-cost discretionary or elective procedures sit as optional riders so the base plan stays affordable.
Preventive dental care is the most heavily covered category in any well-designed group OPD plan, and there's a specific clinical reason. Preventive dental visits don’t necessarily reduce total spend immediately - but they significantly reduce subsequent nonpreventive dental visits and lower nonpreventive dental expenditures, making dental spend more predictable over time. An employer who covers preventive care fully spends less in aggregate on dental than an employer who excludes it - counterintuitive but consistently true in deployment data.
What's typically covered in the preventive category:
What employees should expect: cashless settlement at network clinics for all preventive procedures, with no deductible on most well-structured plans. Pre-authorisation is typically straightforward for preventive care because the clinical evidence requirements are minimal.
Restorative dentistry, fixing teeth that have decay, fracture or other damage, is the highest-frequency claim category after preventive care. Coverage is broad on the base tier of most plans because excluding restorative care defeats the purpose of having dental cover at all.
Covered procedures in this category:
The clinical pre-authorisation requirement on procedures like root canals exists for a specific reason. Root canal claims are frequently submitted in error (a procedure billed as a root canal when only pulp therapy was performed, or vice versa). Pre-authorisation with radiograph evidence catches the discrepancy before payment. On Toothlens-administered plans, AI-driven pre-authorisation completes this review in under 4 hours for routine cases.
Crowns and bridges represent a step up in cost and complexity. Plan design here splits into two patterns:
On standard tiers - Crowns and bridges are often structured as optional riders, not because they aren’t clinically important (they are, especially after root canal treatment), but because their relatively high per-claim cost (₹3,000–25,000+ depending on material, higher for bridges) and classification as major restorative procedures create meaningful cost impact at a population level.
On premium tiers - crowns and bridges are included in the base coverage, often with sub-limits per claim and per policy year.
What employees should know: a crown placed after a root canal is functionally part of the same treatment plan, but is billed as a separate procedure. A plan that covers root canals but excludes crowns leaves the employee with the more expensive part of the treatment uncovered. Premium-tier coverage or a crown rider closes this gap.
Material choices matter for coverage eligibility. Porcelain-fused-to-metal (PFM) crowns are the standard covered option on most plans. All-ceramic and zirconia crowns may be covered at PFM rates with the difference paid by the employee, or covered fully on premium tiers.
Two procedure categories are consistently structured as optional riders rather than base coverage on Indian dental plans, and the reasoning is structural:
Dental implants are high per-procedure cost (₹25,000–60,000 per implant including crown), often elective or partially elective, and asymmetric across employee populations. An employee with a single missing tooth has a fundamentally different claim profile from a population average. Indemnity pricing on a base plan including implants becomes uncompetitive; structuring implants as a rider keeps base premiums accessible while making implant cover available to employees who specifically need or want it.
Orthodontics (braces, clear aligners) is similarly structured because of two characteristics: utilisation skews heavily toward children and young adults, and treatment plans extend across 18–36 months rather than being completed in single visits. This makes traditional claim-by-claim adjudication poorly suited; orthodontic riders typically use lump-sum or staged-payment models instead.
Cosmetic dentistry (veneers, whitening, smile design) is generally excluded from base coverage and from most riders because the procedures are by definition elective. Some custom group plans include cosmetic procedures as a rider option, but this is uncommon.
Two categories that are universally covered but sometimes overlooked when employees evaluate plans:
Pediatric dentistry is covered on most family-inclusive plans. This typically includes preventive care, restorations, pulp therapy on primary teeth, and space maintainers. Plans that include children in coverage should specify the age cut-off (typically 18 or 21).
Emergency dental care like toothache, dental trauma, abscesses requiring urgent treatment, etc. is covered on most plans without the standard pre-authorisation timeline. Cashless settlement is available at network clinics for emergencies. Out-of-network emergency care is typically reimbursable, with documentation requirements.
Three categories sit outside coverage on most Indian group OPD dental plans:
Coverage outside the network clinic i.e. when an employee chooses to receive treatment at a non-network clinic, is typically reimbursable on most plans, but at the network rate rather than the actual cost paid. Cashless settlement requires using a network clinic.
Choosing the right dental plan comes down to asking a few critical questions:
The third question - access - matters in particular. Plans with 30-90 day waiting periods on routine procedures effectively delay care, even when coverage exists on paper. In contrast, plans that enable Day 1 access tend to see higher utilization of preventive and early-stage treatments.
A well-structured plan brings these elements together, ensuring immediate access for high-frequency procedures, meaningful coverage for restorative care, and controlled exposure on high-cost treatments through sub-limits or riders. The goal is not just coverage breadth, but real usability without creating cost volatility at a population level.
It’s also worth noting that tier structures like Standard / Premium / Custom Group are broadly representative, but not universal. Different insurers may use varying tier names, inclusion lists, and sub-limit structures - making it important to evaluate the underlying design rather than relying on labels alone.
—----------------------------------------------------------------------------------------------------------------------------
Toothlens Dental Plans are designed with this balance in mind - offering Day 1 cashless access for standard procedures, while applying longer waiting periods only to select high-cost treatments like implants. If you’re rethinking how dental benefits can drive both utilization and cost efficiency, happy to share how this can be structured for your team.